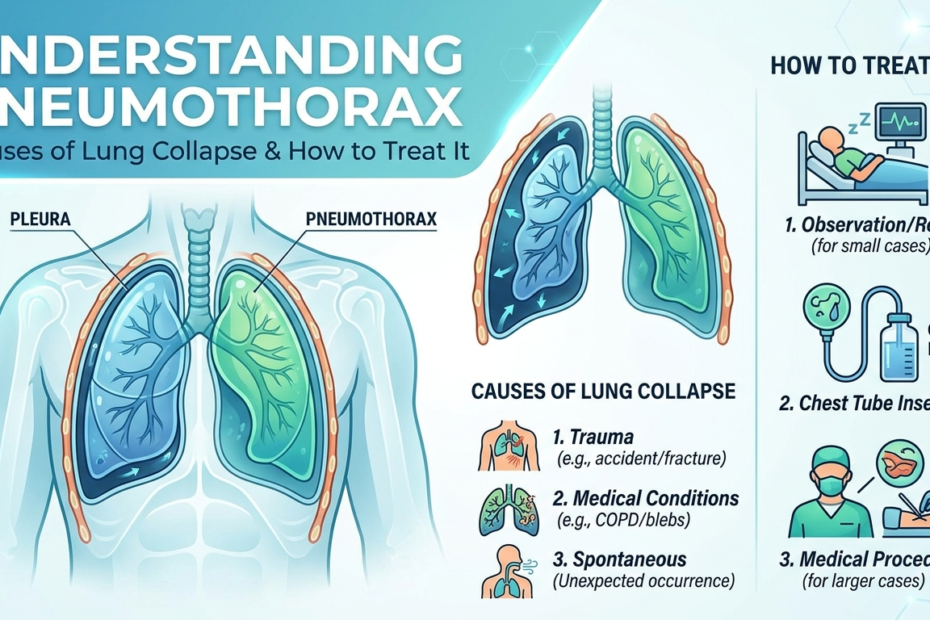
What is pneumothorax becomes a crucial question when someone experiences sudden severe chest pain and breathing difficulty without any obvious cause. This condition occurs when air leaks into the space between the lung and chest wall, causing the lung to collapse partially or completely. The trapped air prevents the lung from expanding normally during breathing, reducing oxygen intake significantly.
The condition ranges from minor cases causing minimal symptoms to life-threatening emergencies requiring immediate medical intervention. Understanding how lung collapse happens and recognizing warning signs allows for prompt treatment that prevents serious complications.
The Different Types of Pneumothorax
The types of pneumothorax fall into distinct categories based on underlying causes and how air enters the pleural space. Spontaneous pneumothorax occurs without any injury or obvious trigger, often affecting tall thin young men without existing lung disease. Small air-filled sacs called blebs on the lung surface rupture spontaneously, allowing air to leak out.
Secondary spontaneous pneumothorax develops in people with existing lung conditions like chronic obstructive pulmonary disease, asthma, cystic fibrosis, or lung infections. Traumatic pneumothorax results from chest injuries penetrating the lung tissue, including rib fractures, stab wounds, or gunshot injuries. Iatrogenic pneumothorax occurs as a complication from medical procedures like lung biopsies or central line placements.
Common Causes of Collapsed Lung in Adults
Pneumothorax causes vary significantly depending on the specific type affecting each patient and their individual health circumstances. Rupture of small air blisters on the lung surface represents the most common cause in otherwise healthy young adults. These blebs form at the lung tops and rupture during normal activities without any identifiable trigger.
Causes of collapsed lung in adults with existing lung disease include damage from chronic inflammation, scarring from previous infections, or emphysema creating weak spots in lung tissue. Mechanical ventilation in critically ill patients can force too much air into lungs, causing rupture. Sudden pressure changes during scuba diving or high-altitude activities sometimes trigger lung collapse in susceptible individuals.
Recognizing the Warning Signs
Pneumothorax symptoms typically begin suddenly with sharp stabbing chest pain on the affected side that worsens with deep breathing or coughing. The pain might radiate to the shoulder on the same side. Shortness of breath develops quickly, ranging from mild breathlessness to severe respiratory distress depending on collapse extent.
Rapid shallow breathing occurs as the body attempts to compensate for reduced lung capacity and oxygen intake. Heart rate increases as the cardiovascular system works harder to maintain oxygen delivery to tissues. Some patients experience anxiety or panic from the frightening sensation of being unable to breathe properly. Severe cases cause bluish skin discolouration from inadequate oxygen levels in blood.
How Doctors Diagnose Lung Collapse
Physical examination reveals decreased breath sounds on the affected side when doctors listen with stethoscopes during breathing. Chest X-rays confirm diagnosis by showing air in the pleural space and the degree of lung compression. The images reveal whether collapse is small, moderate, or complete.
CT scans provide more detailed views when X-rays show unclear results or when doctors need to assess underlying lung disease. Blood oxygen levels measured with finger sensors indicate how severely the collapse affects oxygen delivery throughout the body. These diagnostic tests guide treatment decisions based on collapse severity.
Treatment Approaches for Different Severities
Small pneumothorax cases involving less than fifteen percent lung collapse sometimes resolve without intervention beyond observation and oxygen therapy. Pneumothorax treatment for larger collapses involves inserting a chest tube between ribs to remove trapped air and allow lung re-expansion. The tube connects to a drainage system creating suction that pulls air out continuously.
Collapse of lung treatment continues until the lung fully re-expands and no air leaks persist, typically requiring several days of hospitalisation with the chest tube in place. Recurrent cases or persistent air leaks might need surgical intervention to seal the leak source and prevent future episodes.
Surgical Options for Complicated Cases
Video-assisted thoracoscopic surgery allows surgeons to remove blebs or seal air leaks through small incisions using camera guidance. Chemical pleurodesis involves introducing irritating substances into the pleural space that cause inflammation, making lung surfaces stick to chest wall. This scarring prevents future air accumulation by eliminating the space where air could collect.
Open surgical procedures become necessary when minimally invasive approaches fail or when extensive lung damage requires repair. Pneumothorax treatment decisions balance effectiveness against invasiveness based on individual patient circumstances and likelihood of recurrence.
Recovery Timeline and Expectations
Most patients recover fully after successful treatment with lung function returning to normal levels within weeks. Physical activity restrictions apply initially to prevent recurrence whilst healing completes. Avoiding air travel and scuba diving for several weeks prevents pressure changes from triggering another collapse.
Follow-up chest X-rays ensure the lung remains expanded and no new air accumulation occurs. Smoking cessation becomes crucial for preventing recurrence because tobacco use significantly increases future pneumothorax risk in susceptible individuals.
Preventing Future Episodes
People who experienced one spontaneous pneumothorax face approximately thirty percent risk of recurrence within two years without preventive measures. Surgical interventions substantially reduce this risk to under five percent by eliminating bleb formation sites. Avoiding activities creating sudden pressure changes protects against recurrence in high-risk individuals.
Managing underlying lung diseases through proper medication use and avoiding respiratory infections reduces secondary pneumothorax risk. Understanding pneumothorax causes and personal risk factors allows individuals to make informed decisions about activities and seek prompt care if pneumothorax symptoms develop again.
{kind=link}